English
English Українська
Українська Русский
РусскийDEVICE SENTIERO ADVANCED
Providing maximum flexibility and unparalleled functionality, the SENTIERO ADVANCED offers ABR, ASSR, EABR, ECochG, OAE, air and bone & speech audiometry AND with the SENTIERO ADVANCED Tymp add-on, Class 1 and 2 Tympanometry, providing test capabilities for your clinic in one device.
Neonatal audiometer SENTIERO ADVANCED standard configuration (part number 100340-ED) configuration is supplied with Binaural ABR for both Screening and Diagnostic testing and includes choice of insert earphones or headphones ,electrode cable, bag of 30 electrodes, manual, charger, USB cable, carrying case and MIRA PC Software.
DEVICE SENTIERO SCREENING

The SENTIERO screener is suitable for testing all ages from Newborn and upwards utilizing rapid two frequency simultaneous DPOAE and with the option to add a built-in Pure Tone Screening audiometer. SENTIERO screener is dedicated to perform screening tests with an outstanding test performance based on over 20 years of PATH MEDICAL experience.
Suitable for all ages, SENTIERO screener provides reliable results combined with simple and efficient operation.
DEVICE SENTIERO TYMP SCREENING
The SENTIERO DESKTOP screener provides Tympanometry Class 2 with a combined OAE/Tymp probe and the flexibility to add OAE, Pure Tone and Speech audiometry modules. The standard SENTIERO DESKTOP Class 2 Tympanometer (part number 100497-US1) has ability to do Ipsilateral reflexes and includes Tymp/OAE probe, 2 ear tip starter kits, manual and charger.
DEVICE QSCREEN

QSCREEN® was developed to fit your essential needs in newborn hearing screening with efficiency, accuracy and reliability. It’s a versatile screening OAE and ABR platform incorporating TEOAE & DPOAE including our unique features such as FMDPOAE and multifrequency testing. Furthermore, QSCREEN® offers high performance screening ABR to suit the needs of fast and reliable automated ABR recordings including flexible configurations fully customizable to your NHS program regional protocols
Supplied with the world’s first noise cancellation OAE probe our technology allows OAE testing in noisy environments and significantly reduces your test time. The probe features 2 microphones and reduces the sensitivity of the environmental noise up to 12 dB. This makes the test time up to 50% faster.
Simplify your data entry using QSCREEN’s high definition camera, barcode and QR code detection mechanisms. QSCREEN® is designed to make everyday tasks as easy as possible! Charging, data transfer to the docking station, printing, and modem transfer to pathTrack are all performed wirelessly.
Branches of “Hearing Center” in many cities of Ukraine, such as: Kyiv, Lviv, Chernihiv, Zhytomyr, Kharkiv, Dnipro, Odessa, Ivano-Frankivsk, form a network of establishments providing hearing examination services.
Also, the “Hearing Center” company is engaged in wholesale and retail sales of equipment for the diagnosis of hearing in children and adults: audiometers, impedance meters, devices for registration of OAE, KSVP (ABR), ASSR from the world’s leading manufacturer PATH MEDICAL (Germany).
For the first time otoacoustic emission (OAE) was registered in 1978 by D.T. Kemp (although its existence was predicted a decade before). This gave specialists a new tool to study the structures of the inner ear and, in particular, the microstructure of the organ of Corti.
Otoacoustic emission is a sound signal taken using a sensitive microphone located in the external auditory canal in response to a given sound impulse. Registration of the UAE signal occurs a few milliseconds after the presentation of the sound stimulus. Most likely, otoacoustic emission is the response of the helical structures, which is recorded in the form of acoustic energy.
Research by D.T. Kemp and R. Chum showed that the energy of otoacoustic emission can be greater than the energy of the applied stimulus and suggested that this is due to an active mechanism in the helix of the inner ear. It is believed that the ability of the outer hair cells of the curl to contract brings additional energy to the movement of the basement membrane, thus amplifying the incoming sound signals. Then otoacoustic emission is a by-product of the active process in the helix and, most importantly for practical medicine, can be an indicator of the physiological state of the basement membrane biomechanics.
The source of the induced UAE is the curl, confirmed by its properties:
– the OAE is caused by a physiologically extremely vulnerable, its amplitude is significantly reduced after intense sound exposure, with the use of an ototoxic drug, with hypoxia … This can only be explained by the participation of the biomechanical structures of the curl.
– the amplitude characteristic of the induced OAE is non-linear and belongs to the type of saturation characteristics (at 60 dB RCT). Thus, OAE cannot simply be a reflection of sound in the middle ear.
The discovery of otoacoustic emission made it possible to objectively, non-invasively assess the state of the micromechanics of the curl. Considering that the percentage of patients with sensorineural hearing loss caused by damage to the structures of the curl caused by the influence of noise, ototoxic drugs, and other disorders is quite large, one cannot but pay tribute to the method that allows an objective assessment of the state of the structures of the curl of the inner ear.
Otoacoustic emission is divided into spontaneous and induced.
Spontaneous OAE (SOAE – spontaneous otoacoustic emissions) can be recorded without stimulation. However, it is not used for diagnostic purposes, because it is registered only in 40-50% of young people with normal hearing.
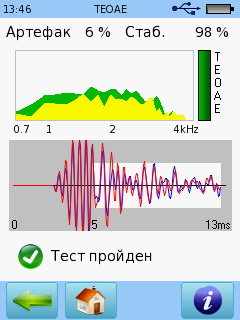
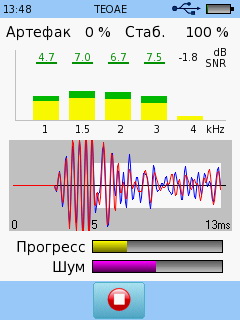
A transiently evoked otoacoustic emissions (TEOAE) is recorded in response to a brief acoustic stimulus. It is registered in people with normal hearing. In cases of sensorineural hearing loss, if the thresholds do not exceed about 25-35 dB (may vary depending on the equipment used), delayed OAE is also recorded.
Stimulus frequency otoacoustic emissions (SFOAE) is recorded during stimulation with a single tonal acoustic stimulus.
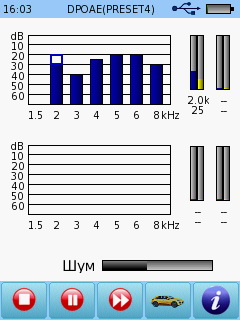
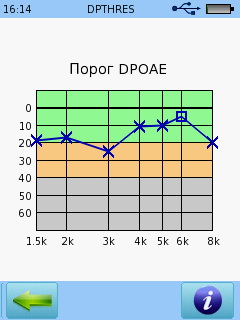
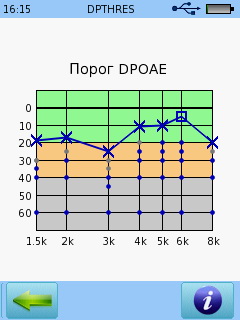
The distortion-product otoacoustic emissions (DPOAE) induced by OAE is recorded when two tone signals with different frequencies f1 and f2 are applied, while the OAE component at the frequency 2f1-f2 has the largest response amplitude. By changing the ratio of the frequencies of the applied signals, it is possible to obtain information about the preservation of the function of the hair cells of any part of the basal membrane of the curl. Registered in people with normal hearing. In cases of sensorineural hearing loss, if the thresholds do not exceed about 45-50 dB (may vary depending on the equipment used), the OAE at the frequency of the observation product should also be recorded.
Since the stimulus signal is delivered to the helix (most often) through the middle ear, and the OAE signal is transmitted from the helix to the ear canal also through the middle ear, its condition greatly affects the characteristics and presence of OAE.
Dysfunction of the middle ear (otitis media, presence of fluid in the tympanic cavity, perforation of the tympanic membrane, other types of conductive component of hearing loss) leads to a decrease in the amplitude and a change in the frequency spectrum of the OAE, up to the impossibility of its registration.
The method of registration of otoacoustic emission is used in the following cases:
• Confirmation of sensorineural hearing loss after neonatal screening.
• Evaluation of auditory function in children at risk (the possibility of congenital hearing loss or a high probability of acquiring it)
• Frequency-specific and quantitative assessment of mild to moderate hearing loss in infants
• Topical diagnostics
• A quick test to get information about rumors in preschool and school age children
• Early detection and monitoring of outer hair cells in the middle ear after exposure to noise or ototoxic drugs
• For medical findings, confirmation of noise-induced hearing loss.
• Identification of persons feigning hearing loss